
1) Welcome to the next installment of our key #oncology meeting highlights via #accredited #tweetorials from @onc_ce, your new (& only) home for the latest education from #experts on #cancer care. #Physicians #nurses #pharmacists #PAs and #NPs all earn 0.5h CE/#CME by following!
2) We continue our coverage of @ASH_hematology 2021 #ASH21, from December! Our expert author is Dr. Ola Landgren @DrOlaLandgren from @SylvesterCancer @univmiami Miller School of Medicine. He is focused on emerging therapies in relapsed & refractory myeloma #RRMM.
3) These #ASH21 summaries on the latest on #multiplemyeloma from @onc_ce & its companion website http://www.oncologytweetorials-ce.com are supported by an educational grant from Abbvie. Content is intended for #healthcare providers. Faculty disclosures are listed at http://www.oncologytweetorials-ce.com/disclosures/.
4) @ash21 was a primary international scientific symposium for interaction & exchange among basic scientists and clinicians working in #HEMATOLOGY #ONCOLOGY #ASH21 was a hybrid meeting this year, with many renowned researchers welcoming the opportunity to collaborate FTF!
5a) Let me start with some foundational info on #MultipleMyeloma–before we move on to new tx. Which of the following statements is FALSE?
a. African Americans have 2-3x⬆️risk of MM
b. African Americans have 2-3x⬆️risk of #MGUS (monoclonal gammopathy of undetermined significance)
5b) (QUIZ, continued)–which is FALSE?
c. Racial disparity in #MGUS & #MM may be due to environmental/socio-economic factors and/or genetic predisposition
d. The median age of onset for #MGUS & #MM is the same in African Americans and Caucasians
6a) Did you vote? Choice d is INCORRECT. The median age of onset for #MGUS and #MM is 5-10 years earlier in African Americans versus Caucasians; causes for that are largely unknown.
6b) The higher risk for African-Americans is there, and it is likely due to a similarly⬆️risk of #MGUS, a precursor condition to #MM. This holds across geography and #SES.
7) As @VincentRK points out, we have a lot of work left to do: Reduce disparities to access to care, finding mechanisms of disparity, improve accrual of African Americans and minorities to clinical trials, improving outcomes.
8) So, on to our first highlight: updated results from the Ph 3 CANDOR trial: #Carfilzomib, Dexamethasone, & #Daratumumab (KdD) vs Carfilzomib/Dexamethasone (Kd) in #RRMM. The original results, https://pubmed.ncbi.nlm.nih.gov/32682484/, showed KdD significantly⬆️PFS versus Kd
9) There was also a favorable benefit–risk profile for KdD. These results were updated at in Lancet Oncology 2022 (https://www.thelancet.com/article/S1470-2045(21)00579-9/fulltext).With approximately 28 months of additional follow-up, a 13.4-month improvement in median PFS . . .
10) . . . was observed in pts treated w/ KdD (28.6 mos) vs pts treated w/ Kd (15.2 mos; HR, 0.59 [95% CI, 0.45–0.78]). Safety remains consistent & KdD cont w/ favorable benefit-risk profile & is an efficacious tx option for pts w/ #RRMM.
New data on left; 2020 data on right:
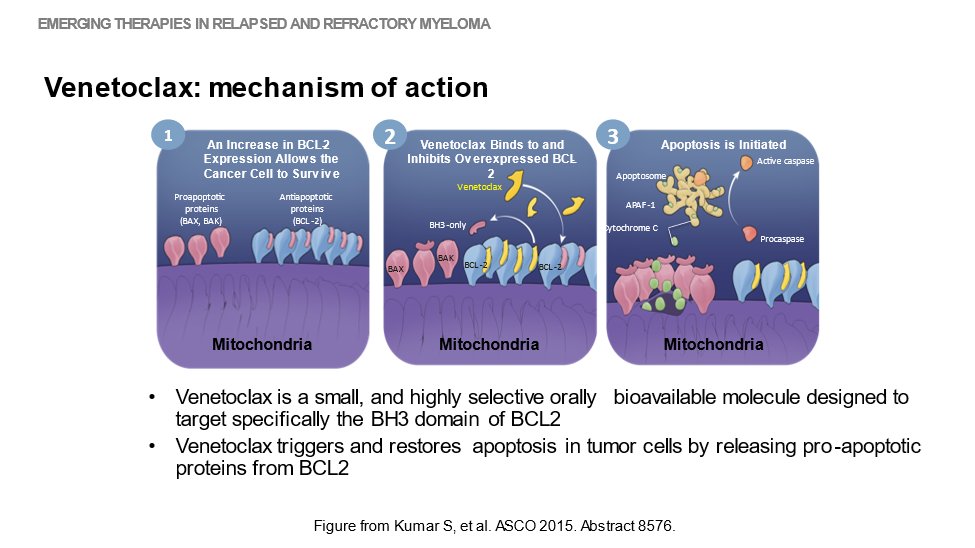
11) Next up–the oral presentation at #ASH21 of the final overall survival results from #BELLINI, a Ph 3 study of #venetoclax or placebo in combo w/ #bortezomib & dexamethasone in #RRMM by Shaji Kumar @myelomaMD from @MayoClinic. Here's the mechanism of action of venetoclax:
12) And here's the study design of BELLINI, as per
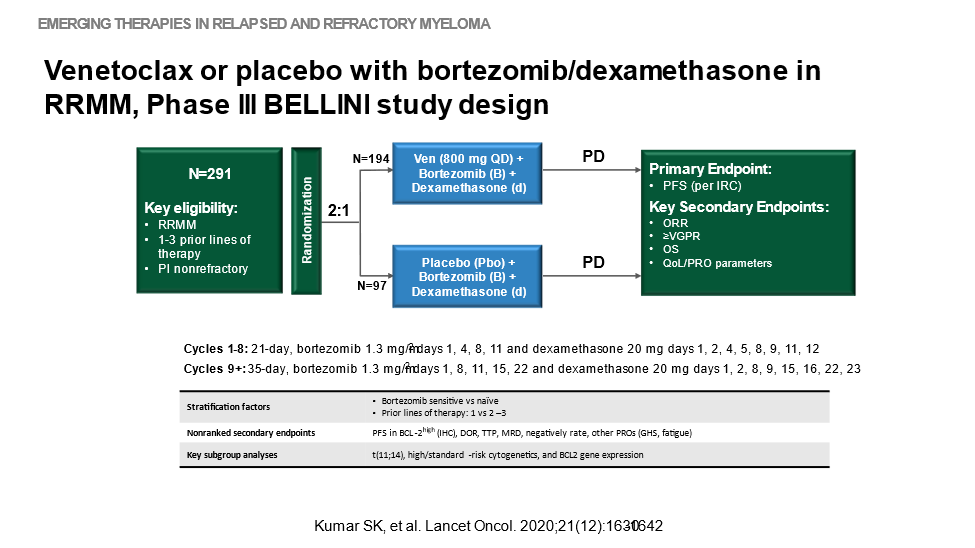
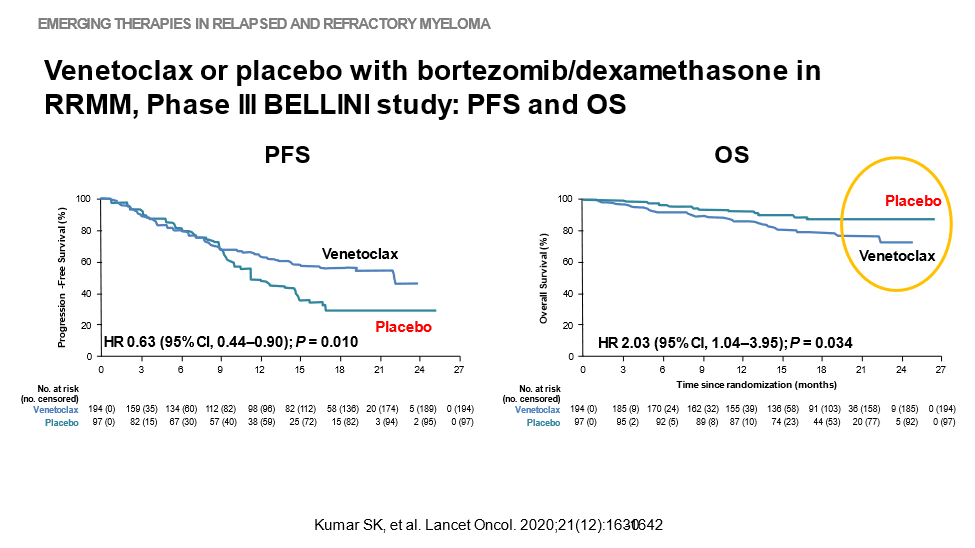
13) The original work ➡️ primary endpoint of PFS per IRC was met with significant improvement w/ venetoclax vs placebo+bortezomib+dexamethasone, but there was⬆️mortality in the venetoclax group, mostly due to⬆️rate of infections ➡️importance of appropriate pt selection
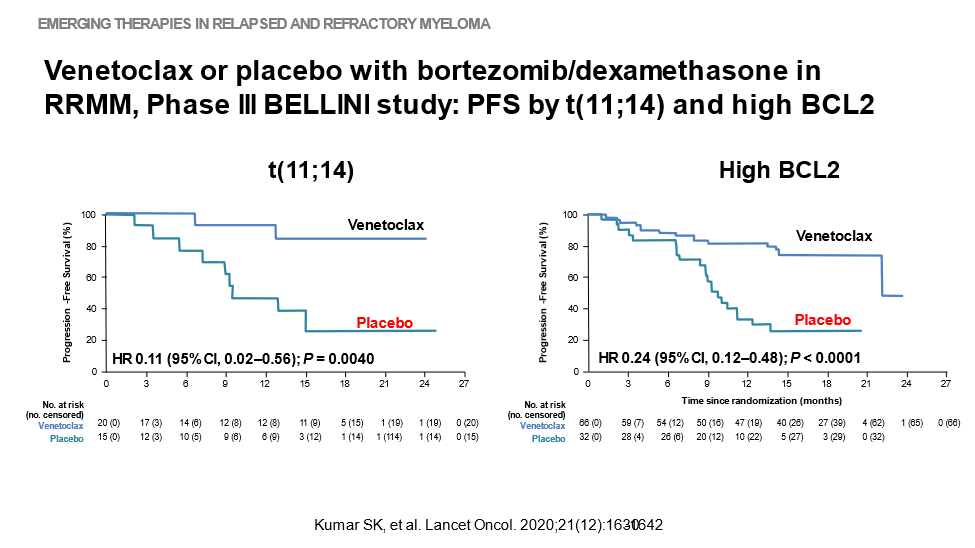
14) Of note, in a subset of patients for whom PFS was measured by t(11;14) and high BCL2, the results (albeit with smaller N) looked different:
15) In the #ASH21 update (🔓https://ash.confex.com/ash/2021/webprogram/Paper145757.html), the addition of Ven to bortezomib & dexamethasone showed significantly improved PFS but resulted in increased mortality versus Pbo in the total population.
16) Consistent with results from previous analyses, Ven added to bortezomib and dexamethasone showed the greatest PFS improvement in pts with t(11;14) or high BCL2, with a favorable benefit-risk profile.
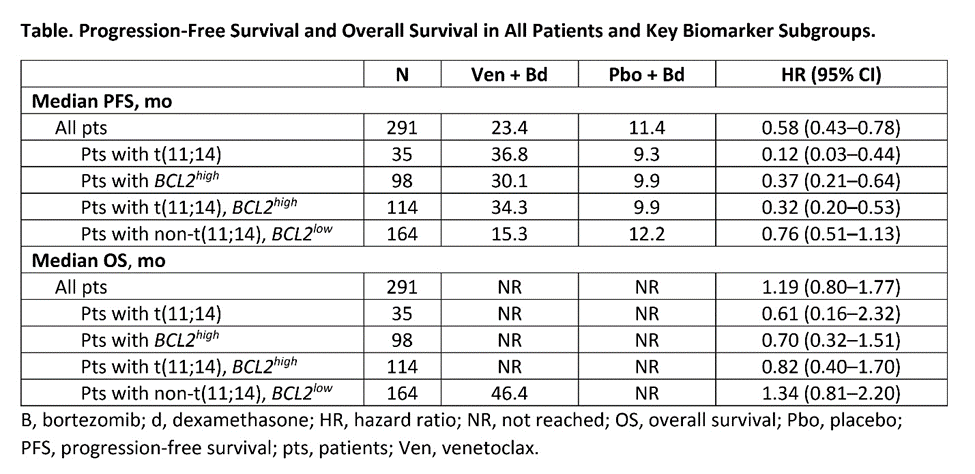
17) @myelomaMD commented: "The data from this trial, as well as additional data from other ongoing venetoclax studies, all point toward the need for us to have a biomarker-driven development strategy for this particular drug, which is what is currently being done."
18) Here's video commentary by @myelomaMD: 🔓
19) So let's pause here, and let me point out that among the Top 10 influencers at #ASH21 (per https://www.symplur.com/healthcare-hashtags/ash21/), fully FOUR are @onc_ce faculty: @SLentzsch @Bethfaiman @SarahCannonDocs (home of our @ErikaHamilton9), and yours truly @DrOlaLandgren.
20) And not to brag, but there WE are–little ol' @onc_ce, which barely launched before #ASH21, in the TOP TEN! All the more reason for you to FOLLOW US, and to RETURN TOMORROW for the remainder of this #tweetorial. Earn that #CME/CE!
21) Welcome back! We're considering advances in treatment of #RRMM from #ASH21. I am @DrOlaLandgren. You're earning CE/#CME!👏to @Rfonsi1 @IreneGhobrial @Myeloma_Doc @MikkaelSekeres @DrMvandenBrink @landau_lab @ninashah33 @NoopurRajeMD @AuclairDan @MalinHultcrantz @sykristinsson
22) What about CAR T for #RRMM? My colleague @SLentzsch introduced you to 🔓https://ash.confex.com/ash/2021/webprogram/Paper145572.html, presented by Sham Mailankody of @sloan_kettering. (You can earn🆓CE/#CME on this at https://oncologytweetorials-ce.com/rrmm_bites_cart/)
23) She discussed that ALLO-715 UNIVERSAL is the first allogeneic anti-BCMA CAR T study to demonstrate safety & substantial efficacy in #MM, and that "off-the-shelf” AlloCAR Ts have potential to address significant unmet need in pts w/rapidly progressive disease.
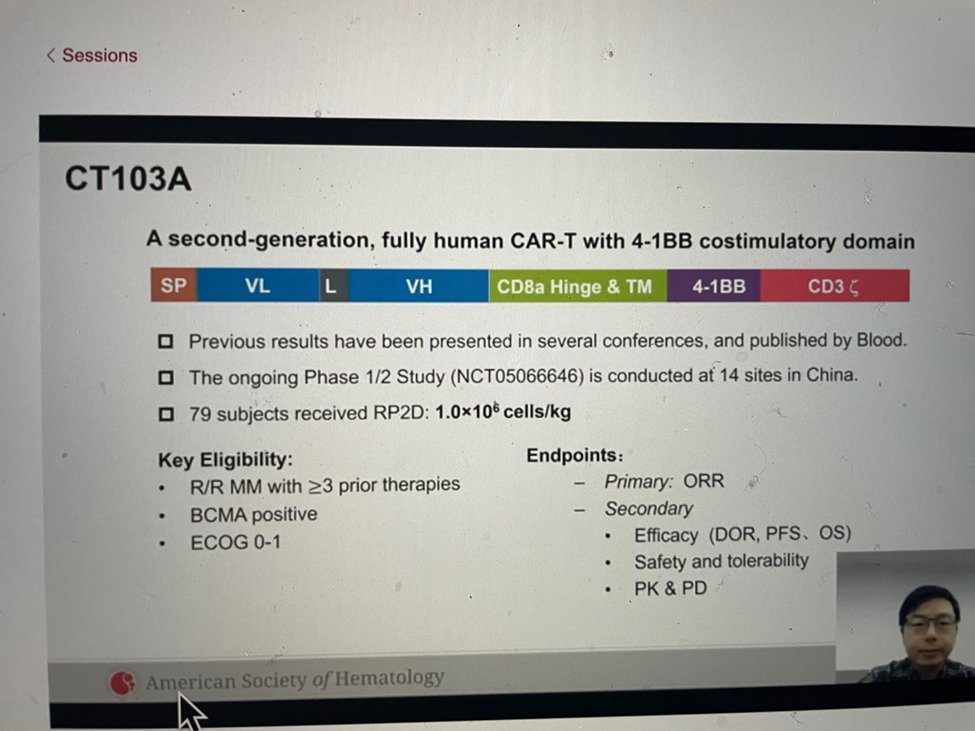
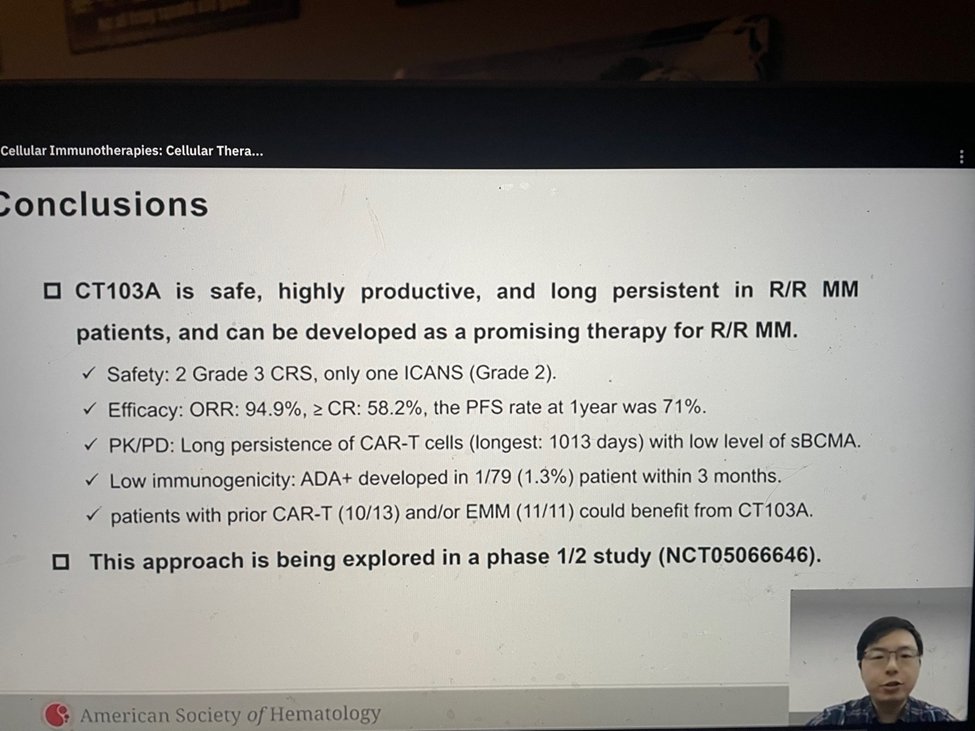
24) Were there other CAR T data for #RRMM released at #ASH21? YES! Check out 🔓https://ash.confex.com/ash/2021/webprogram/Paper152576.html, a Ph 1/2 study of #CT103A, a fully human, BCMA-specific CAR T-cell therapy. CT103A produced durable responses in pts w/#RRMM, even in those who . . .
25) . . . had received prior murine BCMA CAR T-cell therapy, according to Di Wang, MD, PhD, of Tongji Hospital in Wuhan, China. Patients received the recommended phase 2 dose of CT103A (1.0 x 106 cells/kg) after lymphodepletion with fludarabine and cyclophosphamide.
26) For the entire cohort, the ORR was 94.9%, & the CR rate was 58.2%. Among patients who had EMM and/or had received prior CAR T-cell therapy (n=20), ORR was 85.0%, & CR rate was 55.0%. In the entire cohort, 93.7% achieved minimal residual disease (MRD) negativity.
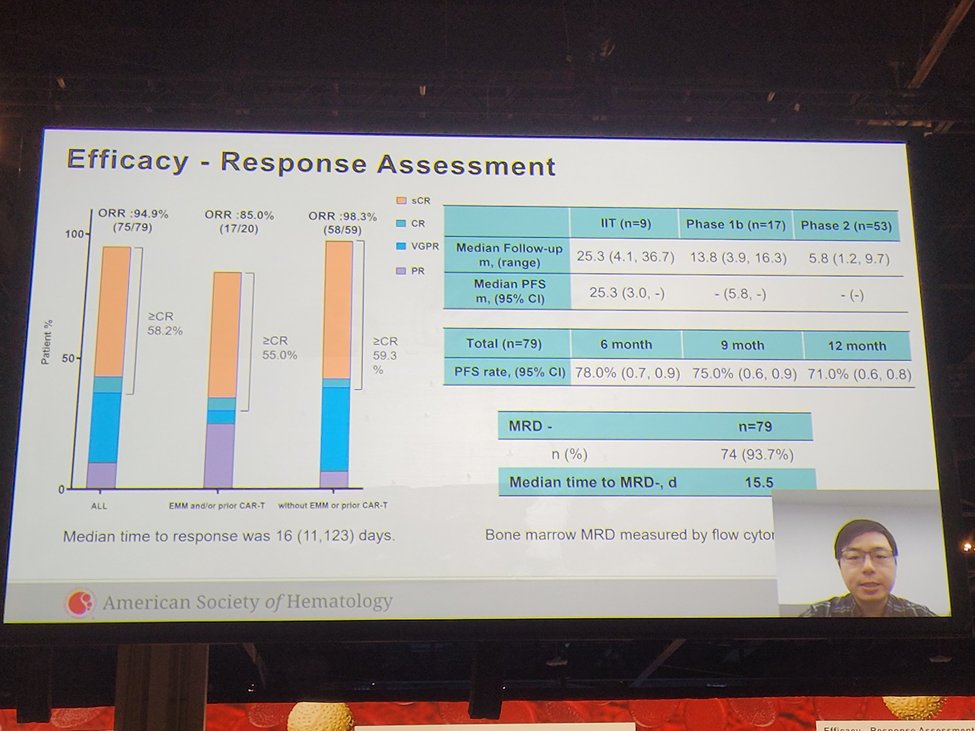
27) The median time to MRD negativity was 15.5 days. Median PFS was 25.3mos. 6-month PFS rate was 78.0%; 12-month PFS 71.0%. CRS was most commonly Gr 1 (64.6%) or Gr 2 (27.8%). No cases of grade 4 or 5 CRS, and 2.5% of patients had grade 3 CRS.
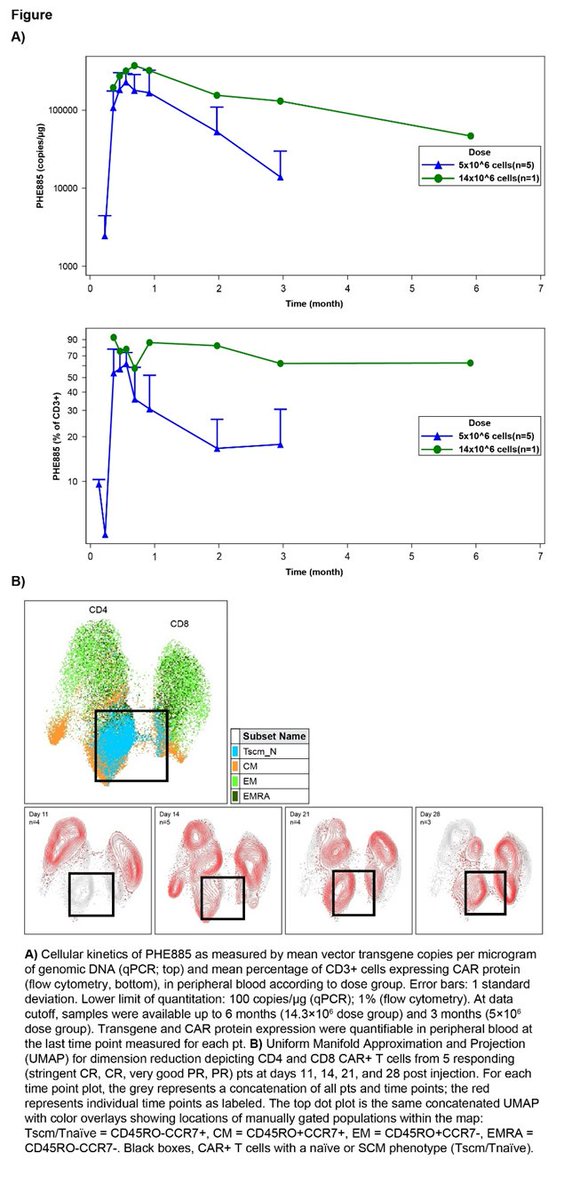
28) And one more: 🔓https://ash.confex.com/ash/2021/webprogram/Paper146646.html, presented by @adamssperling of @DanaFarber, a Ph 1 study assessing #PHE885 manufactured using the T-Charge process & characterization of in vivo expansion, suggesting a preserved T-cell stemness (Tscm) phenotype in pts w/ #RRMM.
29) PHE885 is a unique fully human BCMA CAR-T cell product manufactured using the novel T-Charge platform, which reduces ex vivo culture time to about 24h & takes <2d to manufacture the final product. Pts w/#RRMM to ≥2 prior lines of tx, including …
30) an immunomodulatory drug, proteasome inhibitor, and an anti-CD38 monoclonal antibody, were eligible. Pts received fludarabine & cyclophosphamide for lymphodepletion prior to a single PHE885 IV dose. Primary objectives were safety, including DLTs & AEs.
31a) All pts were heavily pretreated, penta-refractory. There was encouraging clinical activity & manageable safety profile. PHE885 CAR-T cells expand rapidly in vivo, persist at relatively high levels for prolonged periods, and demonstrate a relatively immature T-cell phenotype.
31b) In panel A you see cellular kinetics of PHE885 CAR-T cells. In panel B you see patterns of CD4 and CD8 CAR-T cells in myeloma patients, by depth of clinical response.
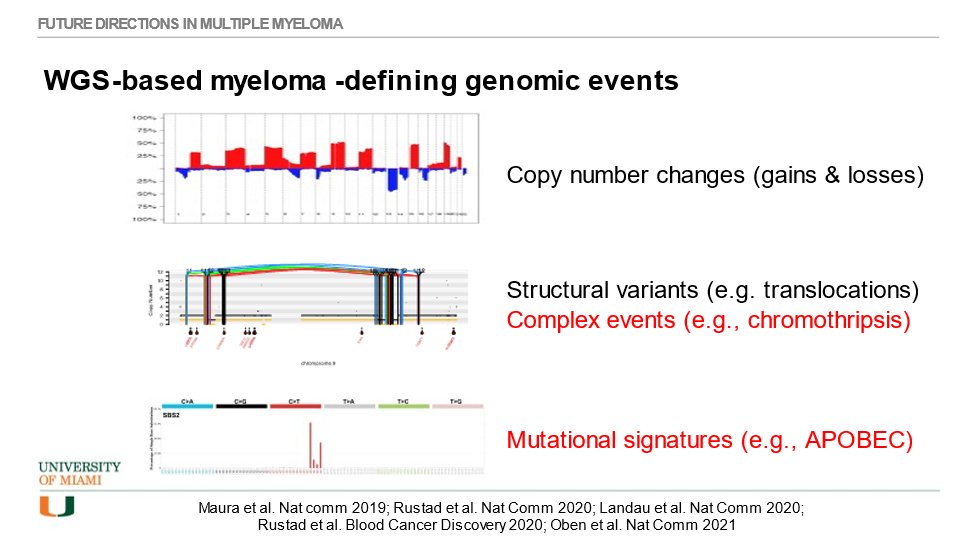
32) Another emerging topic in #MM treatment? Whole-genome sequencing #WGS that is now differentiating between precursor conditions #MGUS vs smoldering myeloma (#SMM) based on myeloma-defining genomic events. I have written about this at 🔓https://pubmed.ncbi.nlm.nih.gov/34889381/.
33) @HadidiSamer kindly tweeted about an #ASH21 educational session on myeloma defining genomic events that I was honored to deliver. Given that most patients with MGUS will not progress to #MM, the potential utility of #WGS is to differentiate progressors from non-progressors.
34) #MM is shaped by a range of myeloma-defining genomic evens. Traditionally, clinicians have looked for IgH translocations and copy number change (gains and losses). But there is much more to discover, and it is clinically very important!
35) A knowledge✅as we prepare to wrap: which of these is NOT true about #chromothripsis
a. literally means "chromosome shattering"
b. likely results from a sequence of mutations
c. occurs through a massive genomic rearrangement during 1 catastrophic event in the cell's history
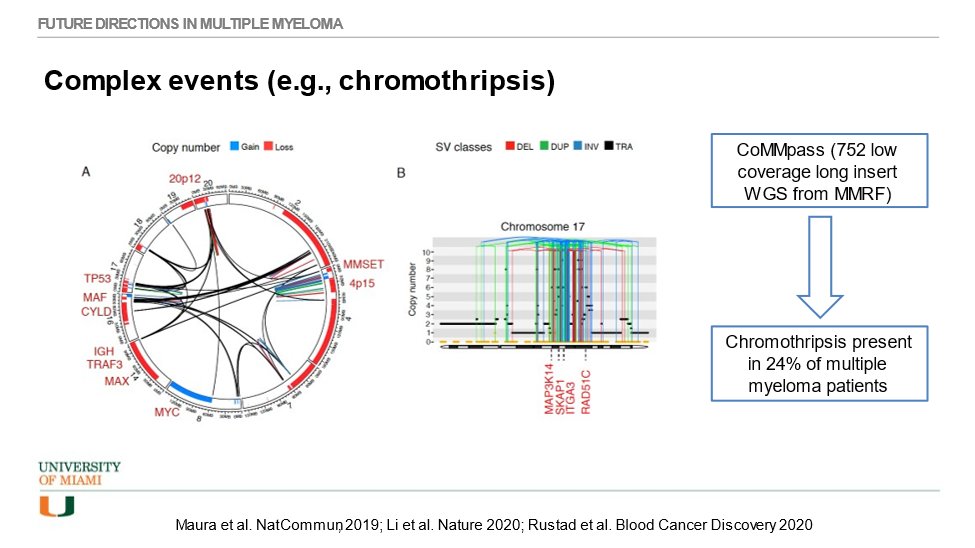
36a) You voted, right? It’s B. Chromothripsis is usually the result of a single catastrophic mutation.
Chromothripsis is a mutational process by which up to thousands of clustered chromosomal rearrangements occur in a single event in localized & . . .
36b) . . . confined genomic regions in one or a few chromosomes. In the large CoMMpass study we have found 24% of all newly diagnosed #MM patients to have chromothripsis; these patients have an inferior prognosis.
37) When studying mutational signatures, we have found #MM to be shaped by 8 distinct signatures. #APOBEC seems to be one of the most important and it can be found to be active in high rates of newly diagnosed patients; it is associated with poorer prognosis.
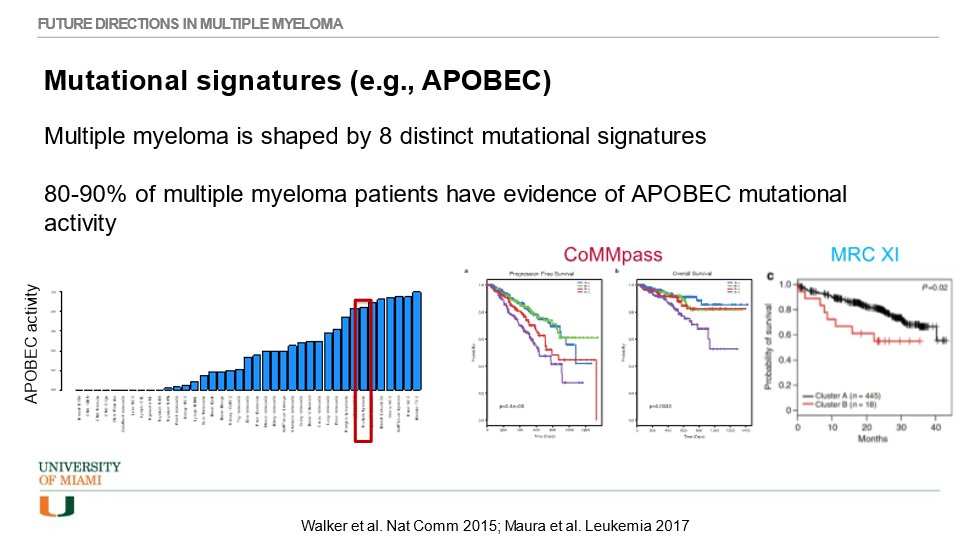
38) Taken together, it is time for the #MM field to move forward with newer & better methodologies to capture difference in disease biology & clinical outcomes. Multivariate analysis show that chromothripsis & APOBEC are independent prognostic factors of PFS & OS . . .
39) … while traditional markers (FISH & cytogenetics) no longer are significant when tested in models including modern assay. Many “high risk” patients (based on old school methods) are truly “standard risk” when treated with modern drugs.
40) We urgently need to implement modern tools to better define high risk patients, and we need to develop rational therapies for such patients. These are important unmet needs!

41) And that's it! You just learned alot about tx for #RRMM and you earned 0.5h🆓CE/#CME 🇺🇸🇨🇦🇪🇺🇬🇧. Just go to https://oncologytweetorials-ce.com/RRMM_emerging to claim your 🆓CE/#CME 🇺🇸🇨🇦🇪🇺🇬🇧. FOLLOW US here @onc_ce for more #accredited #tweetorials by expert authors!🙏@FrancescoMaura4 @LesokhinMD
Originally tweeted by @onc_ce (@onc_ce) on March 24, 2022.